Expand all
Collapse all
Definition
Osteoarthritis refers to a clinical syndrome of joint pain accompanied by varying degrees of functional limitation and reduced quality of life (National Institute for Health and Care Excellence (NICE), 2014). The most affected peripheral joints are the knees, ankles, shoulders, wrist, elbow and joints of the hand and feet. Pain, reduced function, and effects on a person's ability to carry out their day-to-day activities can be important consequences. There is often a poor link between changes visible on an X-ray and symptoms of osteoarthritis: minimal changes can be associated with a lot of pain, or modest structural changes to joints can occur with minimal accompanying symptoms. Contrary to popular belief, osteoarthritis is not caused by ageing and does not necessarily deteriorate (NICE, 2014).
To view the rest of this content login below; or read sample articles.
Symptoms
Osteoarthritis is the most prevalent form of arthritis and a leading cause of pain and disability worldwide (NICE, 2014). In the UK approximately 8.5 million people have joint pain related to osteoarthritis (NICE, 2014). Kloppenburg and Berenbaum (2020) suggested that epidemiological studies are needed to confirm premature mortality in osteoarthritis and its associated physical disabilities.
Osteoarthritis involves degradation of the articular cartilage, synovium, and subchondral bones causing joint pain, functional limitation and reduced quality of life (Cooper et al, 2013). Osteoarthritis can affect any joint. The knee, hip, hand and spine are the most common sites of osteoarthritis – Deshpande et al (2016) estimated that 14 million people in the USA have symptomatic knee osteoarthritis – but it can also occur in the ankles and wrists (Arden and Nevitt, 2006).
Osteoarthritis is characterised pathologically by localised loss of cartilage, remodelling of adjacent bone and associated inflammation (NICE, 2014). A variety
To view the rest of this content login below; or read sample articles.
Risk factors
The risk factors for osteoathritis can be divided into person-level factors, such as age, sex, obesity, genetics, race or ethnicity and diet, and joint-level factors including injury, malalignment and abnormal loading of the joints (Johnson and Hunter, 2014). Age is the single greatest risk factor for the development of osteoarthritis (Shane-Anderson and Loeser, 2010). Women are at greater risk of osteoarthritis and may have more severe symptoms than men, especially after menopausal age (Srikanth et al, 2005). Other risk factors associated with osteoarthritis can be seen in Box 1.
Box 1. Risk factors for osteoarthritis
- Age
- Female sex
- Obesity
- Occupation
- Participation in sports
- Previous injury
- Muscle weakness
- Proprioceptive deficits
- Family history of osteoarthritis
- Acromegaly
- Calcium crystal deposition (Harris and Crawford, 2019).
To view the rest of this content login below; or read sample articles.
Diagnosis
Osteoarthritis can be diagnosed clinically, pathologically, or radiographically (Zhang and Jordan, 2010). Primarily, clinicians may define osteoarthritis by examining the patient's signs and symptoms, and risk factors. According to the NICE (2014) osteoarthritis guidelines:
Osteoarthritis should be diagnosed clinically without investigations if a person: is 45 or over and has activity-related joint pain and has no morning joint-related stiffness, or morning stiffness that lasts no longer than 30 minutes.
Laboratory testing such as inflammatory markers are not usually required to diagnose osteoarthritis. Generally, inflammatory markers, such as erythrocyte sedimentation rate and C-reactive protein level, are normal in osteoarthritis patients (Sinusas, 2012). Radiography such as plain X-rays could be used to confirm the diagnosis. The most common radiographic grading system for osteoarthritis is the Kellgren and Lawrence grade, which scores the severity on a scale of 0–4 – a score of 2 or above indicates definite radiographic osteoarthritis (Kellgren
To view the rest of this content login below; or read sample articles.
Treatment
Recommendations for practice
The goals of osteoarthritis management include pain management and optimal functional ability. To that end, the Osteoarthritis Research Society International has developed patient-focused treatment recommendations for individuals with knee, hip, and polyarticular osteoarthritis (Bannuru et al, 2019).
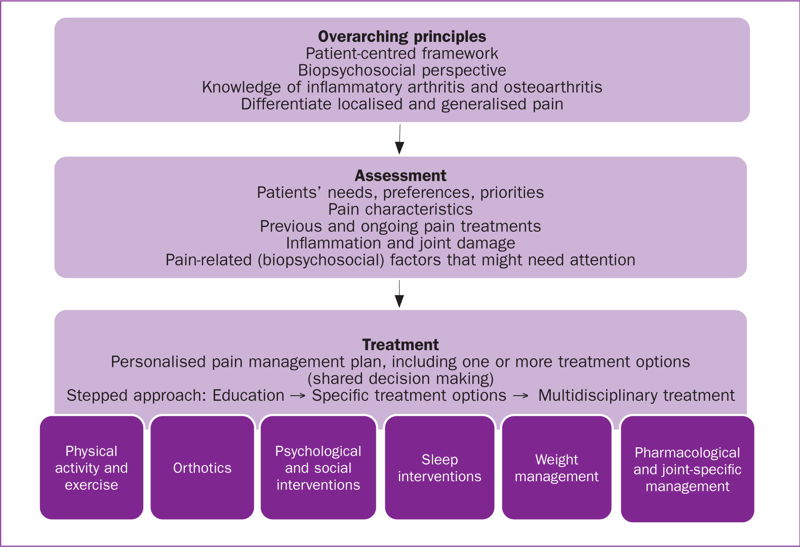
European League Against Rheumatism recommendations for the health professional's approach to pain management in inflammatory arthritis and osteoarthritis are guided by expert opinion and underpinned by a systematic reviews and meta-analyses. An expert group developed and launched the first set of recommendations that enable health professionals to provide knowledgeable and evidence-based pain-management support for people with inflammatory arthritis and osteoarthritis (Geenan et al, 2018) (Figure 1).
To view the rest of this content login below; or read sample articles.
Resources
References
Al-Omari B. Patient preferences for the pharmacological treatment of osteoarthritis using adaptive choice-based conjoint (ACBC) analysis: A pilot study. Eur J Pers Cent Healthc. 2017;5(2):220–224. https://doi.org/10.1007/s40744-017-0056-4
Arden N, Nevitt M. Osteoarthritis: epidemiology. Best Pract Res Clin Rheumatol. 2006;20(1):3–25. https://doi.org/10.1016/j.berh.2005.09.007
Bannuru RR, Osani MC, Vaysbrot EE et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1579–1589. https://doi.org/10.1016/j.joca.2019.06.011
Cooper C, Adachi JD, Bardin T et al. How to define responders in osteoarthritis. Curr Med Res Opin. 2013;29(6):719–729. https://doi.org/10.1185/03007995.2013.792793
Deshpande BR, Katz JN, Solomon DH et al. Number of persons with symptomatic knee osteoarthritis in the US: impact of race and ethnicity, age, sex, and obesity. Arthritis Care Res (Hoboken). 2016;68(12):17. 2016;68(12):1743–1750 https://doi.org/10.1002/acr.22897
Freynhagen R, Geisslinger G, Schug SA. Opioids for chronic non-cancer pain. BMJ. 2013;346: f2937. https://doi.org/10.1136/bmj.f2937
Geenan R, Overman CL, Christensen R et al.. EULAR recommendations for the health professional's approach to pain
To view the rest of this content login below; or read sample articles.