Expand all
Collapse all
Key Points
- Understand the rationale for tracheostomy insertion
- Be able to identify the different types of tracheostomy tube
- Be familiar with contemporary guidelines on tracheostomy care
- Understand the problems that can arise in patients with a tracheostomy and know how to resolve them
To view the rest of this content login below; or read sample articles.
Purpose
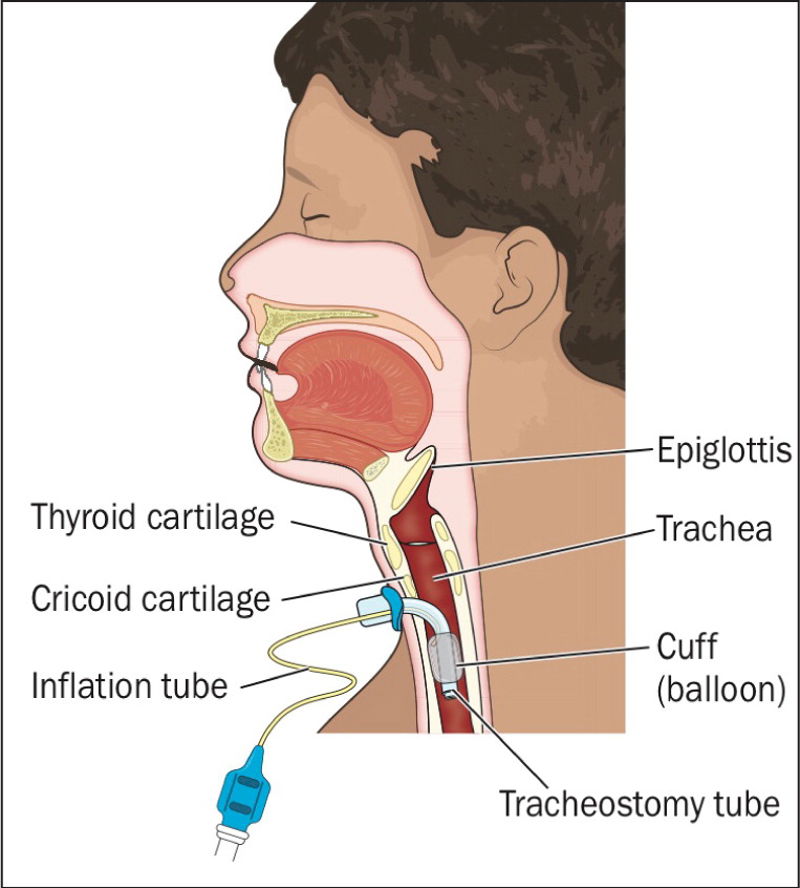
The creation of a surgical airway in the form of a tracheostomy is a common procedure in which an incision is made into the trachea and a tube inserted (Serra, 2000) (Figure 1). Tracheostomies can be temporary or permanent, and are categorised as being either percutaneous or surgical.
It is important for nurses to be able to distinguish between tracheostomies and laryngectomies because, collectively, patients who have undergone these procedures may be referred to as ‘neck breathers’ but there are significant differences in the resultant anatomy (McGrath et al, 2012). A tracheostomy is performed to help patients breathe. A laryngectomy involves the removal of the larynx and separation of the airway from the mouth,
To view the rest of this content login below; or read sample articles.
Assessment
Rationale for insertion
Tracheostomy insertion is rarely a primary procedure and is usually a response to a patient's actual or potential deterioration in clinical condition; it is routinely performed as part of the ongoing management of critically ill patients (Cameron et al, 2009). Despite earlier studies (Arabi et al, 2004; Griffiths et al, 2005; Scales et al, 2008) the Bodenham et al (2014) recognises that early versus late tracheostomy insertion has failed to show benefits from early procedures in terms of a reduction in mortality or hospital length of stay. Indications for placing tracheostomy tubes include: for ventilation, airway obstruction, airway protection, facilitated weaning from mechanical ventilation, and removal of secretions (Morris et al, 2013; Myatt, 2015).
To view the rest of this content login below; or read sample articles.
Equipment
Types of tracheostomy
Tracheostomies can be categorised as either temporary or permanent. A temporary tracheostomy will usually be carried out as an elective procedure to facilitate long-term airway management and the patient will potentially maintain a patent upper airway. A permanent tracheostomy (or laryngectomy) will result in the patient breathing through the stoma for the rest of their life as there is no patent upper airway (Dougherty and Lister, 2015).
Surgical tracheostomies are performed under general anaesthetic and although this procedure has largely been replaced by the percutaneous method, it is still performed on patients undergoing head and neck surgery or those at risk of bleeding (NTSP, 2013; Bodenham et al, 2014). Percutaneous tracheostomy insertion is carried out at the critical care bedside under local anaesthetic, requires fewer resources and may result in less scarring than a surgical insertion. However, in the initial period following insertion, displacement of a percutaneous
To view the rest of this content login below; or read sample articles.
Risks and complications
Nursing care and complications
Tracheostomy insertion allows for a reduction in the use of sedation and patients to be discharged from critical care to general wards. Once discharged from critical care environments, the usual progression is from reliance on the tracheostomy as an airway to mouth breathing and subsequent decannulation (removal). Throughout this trajectory, proficiency in nursing care and interventions is essential to ensure adequate ventilation, oxygenation and communication. Without this specialist level of care, patients are at risk of life-threatening complications. Despite this, research continues to demonstrate that anxiety and a lack of competence among nurses caring for these patients is evident (Day et al, 2002; Freeman, 2011).
Complications can arise following tracheostomy insertion immediately, in the short term or long term. Life-threatening immediate and short-term complications include:
- haemorrhage
- tube blockage through mucous plugging
- accidental tube displacement
Long-term issues include:
- tracheal stenosis (narrowing of the trachea owing to the
To view the rest of this content login below; or read sample articles.
Overview
Providing appropriate suctioning, humidification of inspired oxygen, maintaining a patent inner tube, monitoring cuff pressures and securing of the tracheostomy tube can assist in prevention of immediate and short-term complications associated with tracheostomies. The ‘TRACHE’ care bundle (Hall et al, 2019) identified six main areas of concern when caring for a person with a tracheostomy (Box 1).
Box 1. TRACHE acronym for the six areas of concern in tracheostomy care
- Tapes: keep the tracheostomy tube secure
- Resus/emergency care: know the resuscitation procedure
- Airway clear: use the correct suction technique
- Care of the stoma and neck
- Humidity: essential to keep tube clear
- Emergency equipment (Hall et al, 2019).
Tracheal suction is essential for the removal of secretions from the respiratory tract. Indications for the need for suctioning include audible secretions; reduced oxygen saturation (SaO2), reduced breath sounds, deterioration in arterial blood gases and evidence of cyanosis (Mallett et al, 2013). This
To view the rest of this content login below; or read sample articles.
Resources
References
Dougherty L, Lister S. Tracheostomy and laryngectomy care. In: The Royal Marsden Hospital Manual
To view the rest of this content login below; or read sample articles.